At a glance
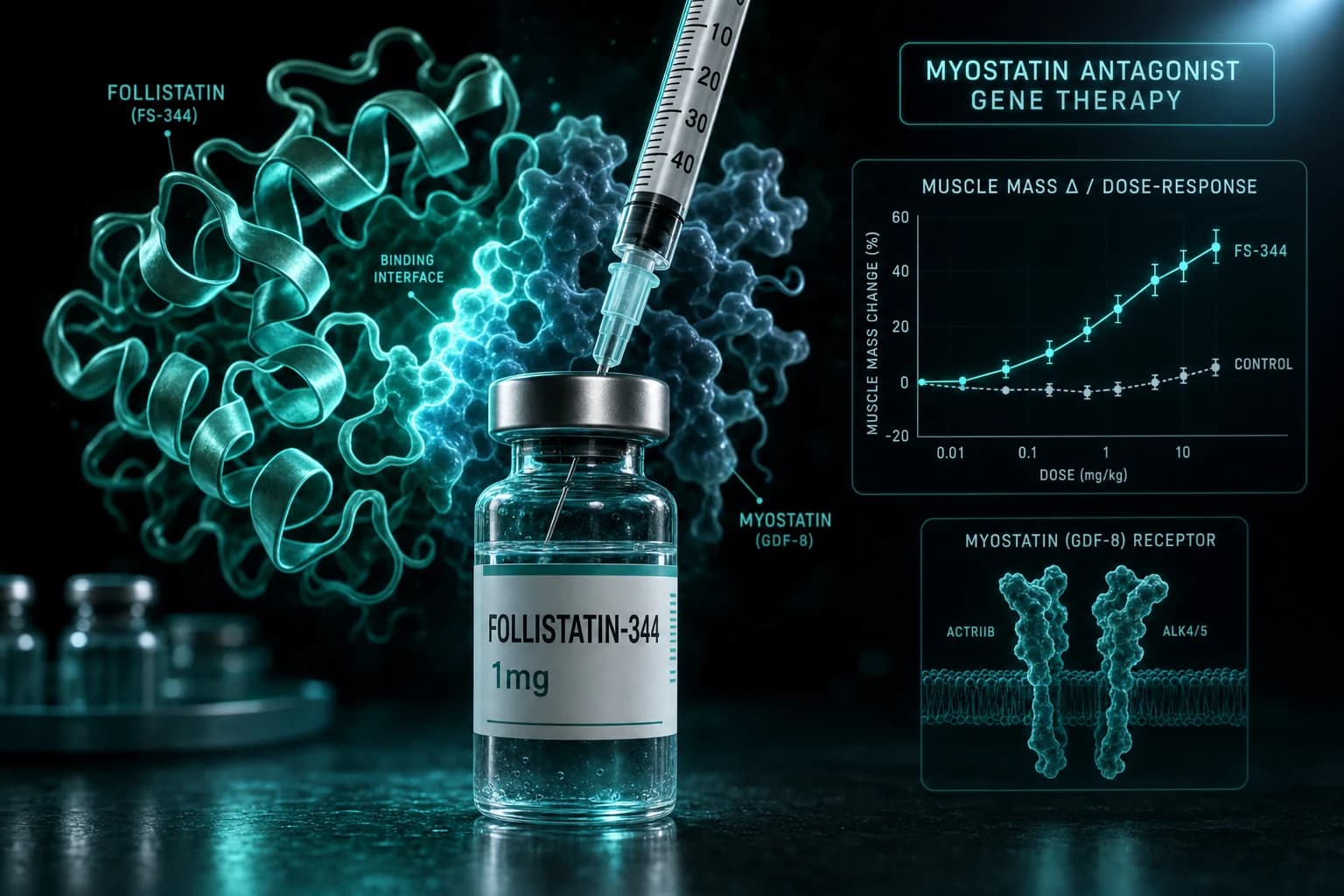
- Follistatin 344 is the 344-amino-acid isoform of human follistatin, an endogenous antagonist of myostatin (GDF-8) and activin
- The strongest published efficacy evidence is for follistatin gene therapy (AAV-delivered FS-344) in mouse, primate, and Phase 1/2 human trials in muscular dystrophy
- Injectable peptide-grade FS-344 has very different pharmacokinetics from gene therapy; serum half-life is short (minutes to hours), unlike the sustained expression from AAV delivery
- Phase 1/2 Becker muscular dystrophy gene therapy trial (Mendell et al., 2017) showed measurable improvement in 6-minute walk distance
- Retail research-grade follistatin peptide does not produce the same systemic myostatin antagonism that AAV-delivered follistatin produces; the comparison is mechanistically misleading
Follistatin 344 is a textbook case of a research compound where the published evidence and the retail product target different versions of the same biology. The clinical efficacy data for follistatin in muscle hypertrophy comes almost entirely from gene therapy trials where AAV vectors deliver sustained expression of follistatin in muscle tissue. Retail "Follistatin 344" peptide injections produce short-half-life systemic exposure that does not replicate the published gene therapy mechanism.
This article covers what follistatin actually is, the strong gene therapy evidence base, the mechanistic case for and against peptide-grade research applications, and what retail follistatin 344 can and cannot do in research protocols.
What follistatin actually is
Follistatin is an endogenous glycoprotein secreted by various tissues including ovary, pituitary, and skeletal muscle. It binds and neutralizes several TGF-β family ligands including myostatin (GDF-8), activin A, and GDF-11. The neutralization effectively removes growth-restricting signaling from muscle and other tissues.
Two major isoforms exist:
| Isoform | Length | Notable property |
|---|---|---|
| Follistatin 288 (FS-288) | 288 amino acids | Higher cell-surface binding affinity; localizes to cell membranes |
| Follistatin 344 (FS-344) | 344 amino acids | Lower cell-surface binding; more freely circulating |
FS-344 is the isoform most-studied in research applications because its circulating profile is more compatible with systemic delivery. FS-288 binds more strongly to cell-surface heparan sulfate proteoglycans and tends to remain locally tissue-bound.
For mechanistic depth, the seminal animal characterization came from Lee et al., PNAS, 2008, which showed follistatin transgenic mice had substantially increased muscle mass through myostatin antagonism.
The gene therapy evidence base
The most-cited follistatin clinical evidence is from gene therapy programs where adeno-associated virus (AAV) vectors deliver sustained follistatin expression in muscle.
Primate proof-of-concept. Kota et al., Sci Transl Med, 2009 demonstrated AAV-delivered follistatin gene therapy in cynomolgus macaques produced sustained muscle hypertrophy without overt off-target effects.
Mouse efficacy. Whittemore et al., 2003 established follistatin as a potent inducer of muscle growth in mouse models. This was before the gene therapy translation.
Human Phase 1/2 in Becker muscular dystrophy. Mendell et al., Mol Ther, 2017 reported the first AAV-follistatin gene therapy human trial in patients with Becker muscular dystrophy. Six-minute walk distance improved at the higher dose levels. The trial was small (6 patients) but demonstrated the gene therapy approach was viable in humans.
Subsequent gene therapy programs. Several biotech sponsors have pursued AAV-follistatin programs for various muscle wasting indications. Programs have advanced and stalled at different stages; the field has remained active through 2024-2026.
Bottom line: The published follistatin evidence base in humans is almost entirely gene therapy. Sustained AAV-delivered expression of FS-344 produces measurable muscle hypertrophy. This is a different mechanism than systemic peptide injection.
Why the peptide form differs
Retail "Follistatin 344" sold by research peptide vendors is typically a synthetic peptide preparation of the follistatin 344 protein. The fundamental challenge:
| Property | AAV-delivered FS-344 (gene therapy) | Injectable peptide FS-344 (retail) |
|---|---|---|
| Tissue concentration | Sustained local expression in muscle | Brief systemic exposure |
| Half-life | Effectively continuous while AAV active | Minutes to hours |
| Muscle delivery | Direct in-tissue synthesis | Depends on uptake from circulation |
| Dose stability | Constant after AAV transduction | Variable peak-and-trough cycle |
The gene therapy approach delivers sustained follistatin expression in the muscle tissue where myostatin is acting. The injected peptide produces a transient peak in circulation that may not achieve effective tissue concentrations during the window where it persists. The mechanism of muscle growth via myostatin antagonism requires sustained suppression, which the peptide injection does not reliably produce.
This is the fundamental reason that retail follistatin 344 peptide protocols often do not produce dramatic muscle hypertrophy results consistent with the gene therapy literature, even at relatively high doses.
What retail FS-344 might still do
The mechanism case for injectable FS-344 having some local effect is not zero:
Local injection effects. Some research protocols inject FS-344 at or near specific muscle groups, hypothesizing local high concentration may produce localized myostatin antagonism even with short systemic half-life.
Combined regimens. Stacking FS-344 with other muscle-growth interventions (testosterone, GH support, training) may produce additive effects even if the FS-344 contribution is modest.
Anti-fibrotic effects. Follistatin has activities beyond myostatin antagonism, including effects on activin A that may contribute to anti-fibrotic outcomes in injured muscle.
What retail FS-344 almost certainly cannot do at typical research-protocol doses: reproduce the gene therapy literature on muscle hypertrophy. The mechanism requires sustained exposure that injection does not deliver.
Standard research protocols
Forum-documented research-grade dosing for retail FS-344 peptide:
| Phase | Dose | Frequency | Route | Duration |
|---|---|---|---|---|
| Common research-use | 100 mcg | Daily or every other day | Subcutaneous | 4-8 weeks |
| Higher-dose | 200-500 mcg | Daily | Subcutaneous | 4-8 weeks |
| Localized injection | 100 mcg | Daily | SC near target muscle | 4-8 weeks |
These doses are extrapolations from rodent studies and from the limited gene therapy clinical data, applied to the substantially different peptide pharmacokinetics. The published efficacy data does not directly support these doses for retail peptide protocols.
For reconstitution math, most retail FS-344 ships as 1 mg vials. Reconstituting with 1 mL bacteriostatic water produces 1 mg/mL. A 0.1 mL draw (10 IU on U-100) delivers 100 mcg.
How FS-344 fits with other muscle-pathway research peptides
| Compound | Mechanism | Evidence base | Practical effectiveness |
|---|---|---|---|
| Follistatin 344 (peptide) | Myostatin/activin antagonism | Strong (gene therapy); thin (peptide) | Limited via injection |
| Follistatin 344 (AAV gene therapy) | Myostatin/activin antagonism | Strong (Phase 1/2) | Substantial; not retail-available |
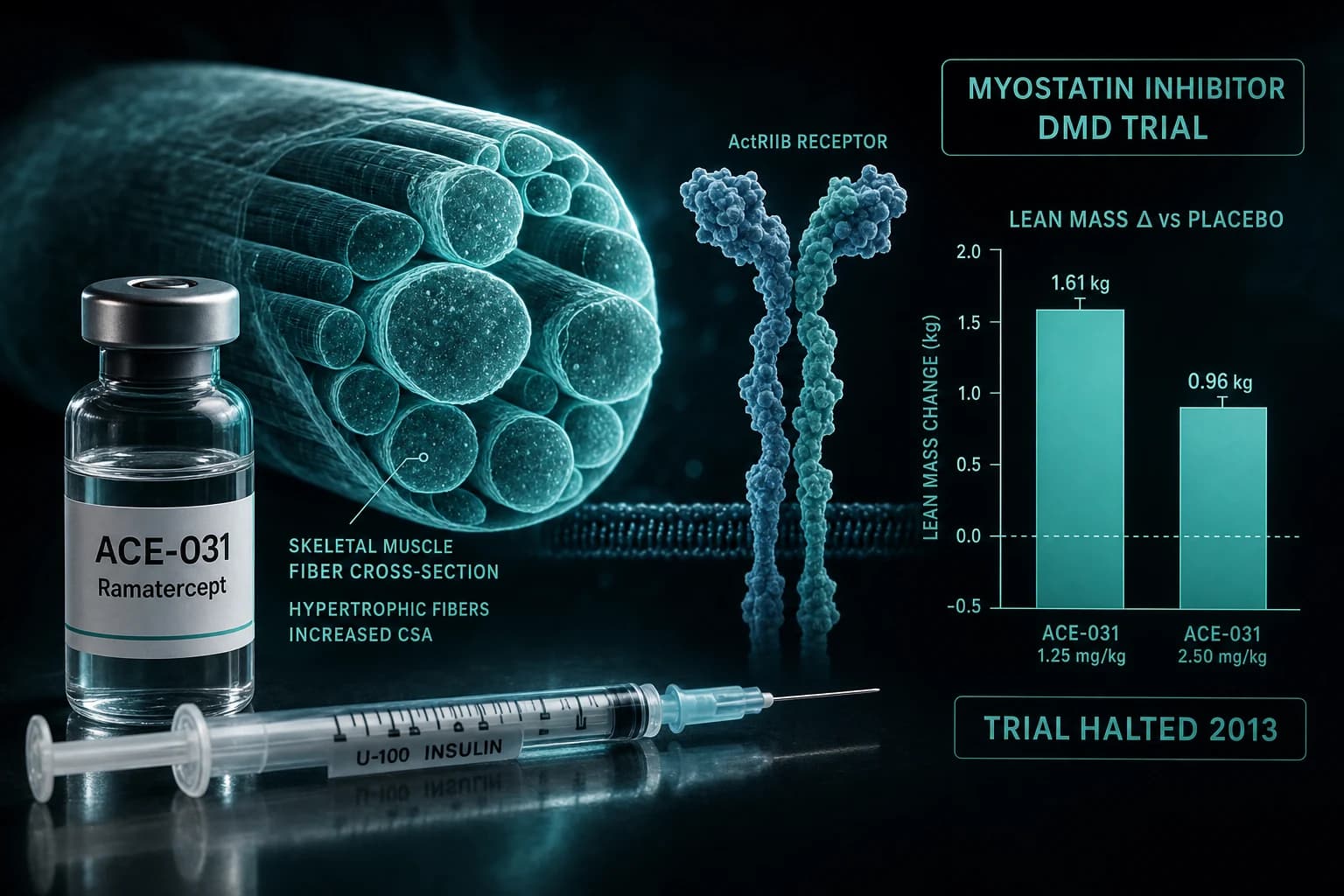
| ACE-031 (ramatercept) | ActRIIB-Fc decoy | Phase 2 halted due to safety | Trial-grade only |
| IGF-1 LR3 | Direct IGF-1 receptor activation | Older trials and animal | Measurable but with risk |
| MK-677 (oral) | GH secretagogue | Long-term oral evidence | Modest body composition shifts |
| BPC-157 + TB-500 | Recovery + angiogenesis | Animal-heavy | Recovery effects, not hypertrophy |
The honest assessment: for muscle-pathway research outside of gene therapy contexts, the directly-translatable peptide options are limited. IGF-1 LR3 targets a different but related pathway with better-characterized peptide-grade effects. The growth hormone secretagogue family targets endogenous GH release rather than direct myostatin pathway.
Sourcing
Research-grade FS-344 peptide is available through some retail peptide vendors. Quality varies significantly because the molecule is complex (344 amino acids) and accurate synthesis requires manufacturer expertise. For research applications targeting muscle hypertrophy via myostatin antagonism, gene therapy products are not retail-available and the peptide-grade alternative has the limitations described above.
For verified-COA research peptides targeting related muscle pathways, see the best legit peptide vendors 2026 ranking.
FAQ
What is follistatin 344?
Follistatin 344 (FS-344) is the 344-amino-acid isoform of human follistatin, an endogenous glycoprotein that binds and neutralizes myostatin (GDF-8), activin A, and GDF-11. Neutralizing these growth-restricting ligands removes the brake on muscle growth and supports muscle hypertrophy.
Does follistatin 344 actually build muscle?
In gene therapy contexts (AAV-delivered sustained expression in muscle), yes. The Phase 1/2 trial in Becker muscular dystrophy showed measurable functional improvements (Mendell et al., 2017). In injectable peptide form at typical research-protocol doses, the evidence is much weaker because the pharmacokinetics do not reproduce the gene therapy mechanism.
What is the difference between FS-344 and FS-288?
Both are isoforms of human follistatin. FS-288 (288 amino acids) has higher binding affinity to cell-surface heparan sulfate proteoglycans and localizes to cell membranes. FS-344 (344 amino acids) has lower cell-surface binding and circulates more freely. FS-344 is the more-studied isoform for systemic muscle-growth research applications.
Is follistatin gene therapy approved?
No. Several AAV-follistatin gene therapy programs have been in development for various muscle wasting indications, but no follistatin gene therapy has reached US FDA approval as of May 2026. Phase 1/2 trials have been conducted with positive efficacy signals at small scale.
Can I get follistatin gene therapy?
No. AAV-delivered follistatin gene therapy is investigational and not commercially available. Trial participation may be possible for patients with specific conditions like Becker muscular dystrophy through clinical trial enrollment.
What is the standard FS-344 peptide research dose?
Forum-documented research dosing is typically 100 mcg daily subcutaneous for 4-8 weeks. Higher doses (200-500 mcg) are sometimes used. These doses are extrapolations from animal data and from gene therapy clinical data applied to substantially different pharmacokinetics; the published evidence does not directly support these doses for peptide-grade injection.
What about combining FS-344 with other compounds?
Stacking with testosterone, GH support, or training interventions is sometimes used in research protocols. Whether the FS-344 contribution adds measurable benefit on top of these established interventions is not characterized in published literature. Most stack rationales are mechanism extrapolation rather than tested combinations.
Further reading
- ACE-031 (ramatercept) myostatin inhibitor research review
- IGF-1 LR3 research dosing protocol
- Sermorelin vs CJC-1295 vs Ipamorelin comparison
- Hexarelin GHRP dosing and cortisol risk guide
- Wolverine Stack: BPC-157 + TB-500 recovery protocol
- Best legit peptide vendors 2026
- MK-677 (Ibutamoren) oral GH secretagogue guide
This article is for educational and research purposes only. Follistatin 344 in peptide form is sold under research-use disclosures and is not approved by the FDA for any indication. AAV-follistatin gene therapy is investigational and not commercially available. None of the content above constitutes medical advice.