At a glance
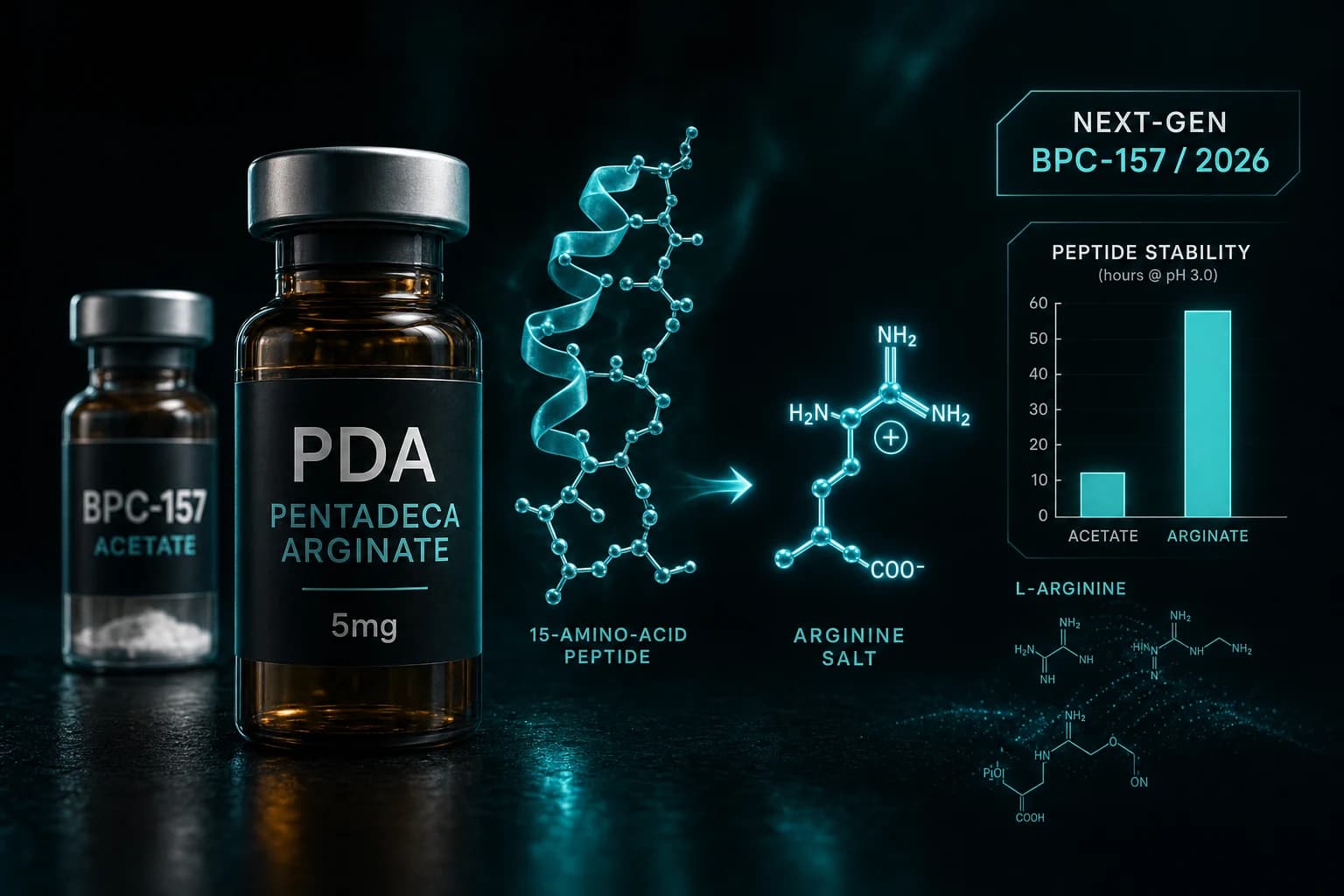
- PDA is the same 15-amino-acid BPC-157 sequence bound to an L-arginine salt instead of the traditional acetate salt
- Oral stability at pH 3.0 is approximately 1,000x higher than BPC-157 acetate; for subcutaneous injection the stability difference is largely irrelevant
- PDA was developed in part as a response to early-2025 FDA compounding restrictions; the Feb 2026 reclassification restored BPC-157 acetate access in parallel
- Standard research dose: 250-500 mcg daily subcutaneous, matching the BPC-157 protocol; oral PDA capsules use 500 mcg to 1 mg per dose
- Published direct evidence for PDA itself is thin; the mechanistic case rests on BPC-157 evidence applied to the arginate salt formulation
Pentadeca arginate is the same 15-amino-acid BPC-157 sequence with one structural change: the peptide is bound to an L-arginine salt instead of the traditional acetate. The change is small at the molecular level but meaningful at the formulation level. The arginate salt is approximately 1,000 times more stable at low pH, which matters for oral bioavailability through the acidic stomach environment.
This article covers what PDA actually is, why the arginate salt matters (and when it does not), the published evidence picture as of May 2026, the standard research dose protocols, and how PDA fits the post-reclassification compounding landscape.
What PDA actually is
BPC-157 is a synthetic 15-amino-acid peptide derived from a sequence in human gastric juice. It is sold as a research compound and is one of the most-discussed peptides in recovery research. The traditional formulation pairs the peptide with an acetate counter-ion, producing BPC-157 acetate.
Pentadeca arginate pairs the same 15-amino-acid sequence with an L-arginine counter-ion instead of acetate. The peptide sequence is identical. The salt form is different.
| Property | BPC-157 acetate | PDA (BPC-157 arginate) |
|---|---|---|
| Peptide sequence | Pentadecapeptide (15 amino acids) | Same |
| Counter-ion | Acetate | L-arginine |
| Molecular weight (incl. salt) | ~1,419 Da | Slightly higher |
| pH 3.0 stability (oral) | Limited | ~1,000x improved |
| Subcutaneous injection stability | Adequate | Equivalent |
| Mechanism of action | Same parent peptide mechanism | Same parent peptide mechanism |
The arginate salt offers meaningful gains for oral dosing because the stomach pH (2-4) is the most aggressive degradation environment most orally dosed peptides encounter. For subcutaneous injection, the peptide bypasses the GI tract entirely and the salt form stability difference is largely irrelevant.
The practical implication: PDA is most differentiated from BPC-157 acetate when used orally. For injectable research-grade dosing, the two formulations should produce similar systemic peptide concentrations once the salt dissociates in vivo.
Why PDA was developed
Three factors drove the arginate-salt formulation into the spotlight in 2024-2025.
FDA Category 2 listing. In late 2024, the FDA placed several research peptides including BPC-157 in Category 2, restricting compounding-pharmacy access. Pharmacies and pharmaceutical chemists had been working on alternative salt formulations as a potential regulatory workaround. PDA was already in development when the Category 2 designation hit.
Marketing differentiation. "Next-generation BPC-157" makes for cleaner marketing than "the same peptide with a different salt." PDA was positioned by some retailers as a meaningfully different compound, even though the active peptide sequence is identical.
Genuine oral bioavailability advantage. The arginate salt does survive gastric pH meaningfully better than the acetate form. For oral protocols specifically, this is a real reformulation advantage, not just a marketing claim.
The February 27, 2026 HHS reclassification moved BPC-157 (and 13 other peptides) back to Category 1, restoring legal compounding-pharmacy access to the parent compound. PDA's regulatory-workaround rationale is now less relevant. The oral bioavailability case remains.
For the broader regulatory context, see the FDA 503A peptide compounding review.
What the published evidence actually shows
This is where the honest framing matters. Direct published evidence for PDA specifically is thin. The mechanism case rests on the parent BPC-157 literature applied to the arginate salt formulation.
BPC-157 evidence base (transferable to PDA):
The strongest BPC-157 evidence comes from preclinical animal models of wound healing, tendon repair, and ulcer healing. Sikiric et al., 2010-2020 review series covers the angiogenic and tissue-repair mechanism in rodent models. The most-cited tendon healing study is Cerovecki et al., 2010, J Orthop Res, which showed BPC-157 accelerated medial collateral ligament healing in rats.
Direct PDA evidence:
A 2024 narrative review (PMC12446177) noted that despite widespread retail availability, published human evidence for BPC-157 (either acetate or arginate form) remains limited. A systematic review screened 544 papers and found 36 met inclusion criteria, with 35 in rodents or cells and only one involving humans.
PDA-specific in vitro stability studies have been published by compounding chemists, demonstrating the pH 3.0 stability advantage. Head-to-head efficacy comparisons of PDA versus BPC-157 acetate at matched bioavailable doses have not been published in peer-reviewed research as of May 2026.
Bottom line: PDA is BPC-157 in a more orally stable salt form. The peptide does the same thing in the body. Most of the "PDA evidence" is BPC-157 evidence with the arginate salt rationale layered on top.
The standard research protocol
For research-grade dosing, PDA protocols largely mirror BPC-157 acetate protocols. The convergent doses:
| Route | Dose | Frequency | Duration |
|---|---|---|---|
| Subcutaneous injection | 250-500 mcg | Once daily | 4-8 weeks |
| Oral (PDA-specific advantage) | 500 mcg to 1 mg | Once or twice daily | 4-8 weeks |
| Localized SC near injury | 250 mcg | Once daily | 2-4 weeks |
The subcutaneous protocol is the same as the BPC-157 dosing protocol guide. Use a 31-gauge insulin syringe, inject into abdominal subcutaneous fat, and run a 4-8 week cycle.
The oral protocol is where PDA offers a real advantage over BPC-157 acetate. The arginate salt's pH 3.0 stability means more of the orally dosed peptide reaches systemic circulation. The published animal work on oral BPC-157 (in the acetate form) showed some gut-targeted effects but limited systemic absorption. PDA oral capsules likely produce higher systemic levels at matched mg doses.
For reconstitution math, the standard 5 mg vial reconstitutes with 1 mL bacteriostatic water for 5 mg/mL concentration. A 0.05 mL draw (5 IU on a U-100 insulin syringe) delivers 250 mcg. The reconstitution calculator handles arbitrary vial sizes.
PDA versus BPC-157 acetate: when each makes sense
| Use case | Recommended formulation | Reason |
|---|---|---|
| Subcutaneous injectable for tendon, ligament, joint research | Either (BPC-157 acetate often cheaper) | Salt form irrelevant after dissociation in vivo |
| Oral protocol for GI healing research | PDA arginate | Better pH 3.0 stability through stomach |
| Research replicating published rodent work | BPC-157 acetate | All published animal data used the acetate form |
| Stack with TB-500 (Wolverine Stack format) | BPC-157 acetate | Pre-mixed combination products use acetate |
The retail pricing for PDA versus BPC-157 acetate varies by vendor. Some vendors price PDA at a premium (10-30% above acetate). Other vendors price them equivalently. For injectable research where the salt form makes little practical difference, the lower-priced option is generally the rational choice.
For oral research specifically, PDA's stability advantage is the legitimate differentiator. For everything else, the choice between salt forms is mostly a marketing preference.
Stacking with related compounds
PDA can be stacked with the same compounds that BPC-157 is commonly stacked with in research protocols.
-
PDA + TB-500: Same mechanistic logic as the Wolverine Stack. BPC-157 (or PDA) drives local growth factor and angiogenesis; TB-500 drives systemic cell migration. Standard dosing pairs PDA 250-500 mcg daily with TB-500 2.5 mg twice weekly.
-
PDA + GHK-Cu: Adds matrix remodeling and collagen synthesis. Used in GLOW Blend format research for skin and connective tissue endpoints.
-
PDA + Thymosin α-1: Combines tissue repair with immune modulation. See the Thymosin α-1 + BPC-157 combined immune recovery protocol for the mechanism case.
-
PDA + KPV (oral protocol): For gut-focused research, the oral PDA stability advantage combined with KPV's PepT1-mediated absorption produces a clean two-compound oral protocol. See the KPV oral peptide gut inflammation research article.
How PDA fits the 2026 regulatory landscape
The February 27, 2026 HHS reclassification moved BPC-157 from FDA Category 2 back to Category 1, restoring legal compounding-pharmacy access. PDA was not separately listed because it is mechanistically the same peptide as BPC-157, just in a different salt form.
The practical implication: both formulations are now accessible through licensed compounding pharmacies with a prescription. The choice between them is increasingly a formulation question (oral vs injectable, marketing preference, pricing) rather than a regulatory access question.
For research-grade applications outside the compounding pharmacy pathway, both formulations remain available through retail peptide vendors with research-use disclosures.
Bottom line: The Feb 2026 reclassification made PDA's regulatory-workaround rationale obsolete. The oral bioavailability case remains the legitimate differentiator. For everything else, PDA is BPC-157 with a different salt form.
Sourcing
For research-grade injectable PDA and BPC-157, Ascension Peptides ships injectable vials with public per-batch COAs and 50% off using code ENHANCED. For oral PDA capsules specifically, Limitless Biotech ships oral peptide capsules with code ENHANCED.
For our broader sourcing analysis including how to verify COAs across vendors, see the best legit peptide vendors 2026 ranking and the where to buy BPC-157 with COAs guide.
FAQ
Is PDA the same as BPC-157?
The peptide sequence is identical (15 amino acids, the pentadecapeptide isolated from human gastric juice). The salt form is different: PDA uses an L-arginine counter-ion while traditional BPC-157 uses acetate. In the body, after the salt dissociates, the bioactive peptide is the same molecule in both formulations.
Is PDA better than BPC-157?
For subcutaneous injection, the two formulations are functionally equivalent because the salt form dissociates in vivo and the same peptide ends up in circulation. For oral dosing, PDA has approximately 1,000-fold better pH 3.0 stability, which translates to better gastric survival and higher oral bioavailability. The "better" question depends on which route you are using.
What is the standard PDA research dose?
Subcutaneous: 250-500 mcg once daily, mirroring the BPC-157 acetate protocol. Oral: 500 mcg to 1 mg once or twice daily, taking advantage of the arginate salt stability. Cycle duration is typically 4-8 weeks across both routes.
Why was PDA developed?
Three factors: (1) the late-2024 FDA Category 2 listing of BPC-157 created regulatory pressure to develop alternative salt formulations, (2) the arginate salt offers genuine oral bioavailability advantages, and (3) "next-generation BPC-157" makes for cleaner retail marketing than "the same peptide in a different salt."
Is PDA legal?
Yes. The February 27, 2026 HHS reclassification moved BPC-157 back to FDA Category 1, restoring legal compounding-pharmacy access to the parent peptide. PDA, being structurally the same peptide in a different salt form, is accessible through the same pathways. Research-grade retail PDA is also available with research-use disclosures.
Can I use PDA alongside the Wolverine Stack?
The Wolverine Stack is BPC-157 + TB-500 pre-mixed in injectable form. PDA is the arginate salt of BPC-157. Adding additional injectable BPC-157 (in either salt form) on top of the Wolverine Stack would double-dose the BPC-157 component, which is not the typical protocol. If you want oral plus injectable coverage, run the Wolverine Stack injectable plus oral PDA capsules for the additional GI-targeted research benefit.
Does PDA have its own published trials?
Direct published trials of PDA specifically (against BPC-157 acetate or against placebo) are limited as of May 2026. Most of the evidence base is BPC-157 evidence applied to the arginate formulation. In vitro stability studies have been published by compounding chemists. Head-to-head efficacy trials at matched bioavailable doses have not been published in peer-reviewed venues.
Further reading
- BPC-157 compound guide
- BPC-157 dosing protocol guide
- Where to buy BPC-157 with COAs
- Wolverine Stack: BPC-157 + TB-500 recovery protocol
- BPC-157 vs TB-500: recovery peptides comparison
- KPV oral peptide gut inflammation research
- FDA 503A peptide compounding review July 2026
- Best legit peptide vendors 2026
- Reconstitution Calculator
This article is for educational and research purposes only. Pentadeca arginate and BPC-157 are sold under research-use disclosures and are not approved by the FDA for any indication outside of established compounding-pharmacy formulations. None of the content above constitutes medical advice. Consult a qualified clinician for individual medical questions.