At a glance
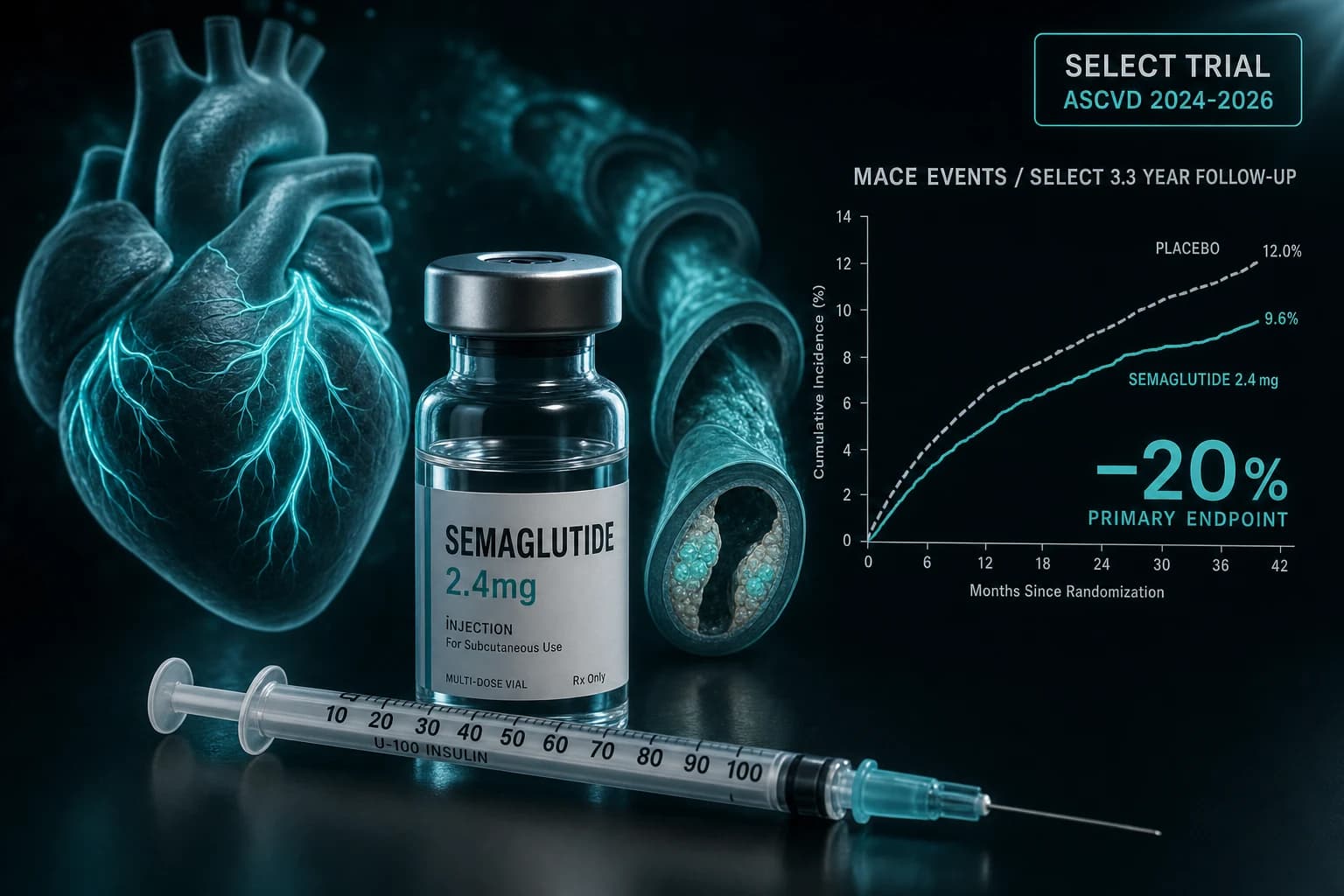
- SELECT (Lincoff NEJM 2023, PMID 37952131): semaglutide 2.4 mg cut MACE 20% versus placebo (6.5% vs 8.0%, HR 0.80, 95% CI 0.72 to 0.90)
- 17,604 adults aged 45 or older with established cardiovascular disease and BMI 27 or higher, no diabetes; mean follow-up 39.8 months
- Deanfield Lancet 2025 (PMID 41138739): only about a third of the MACE benefit is mediated by waist-circumference change
- Deanfield Lancet 2024 (PMID 39181597): the 4,286 patients with baseline heart failure had a larger relative MACE reduction (HR 0.72)
- Colhoun Nature Medicine 2024 (PMID 38796653): pre-specified kidney composite was lower with semaglutide (1.8% vs 2.2%, HR 0.78)
The 20% number is real. The why is the more interesting question.
SELECT randomized 17,604 adults with established cardiovascular disease and a BMI of 27 or higher, no diabetes, to once-weekly semaglutide 2.4 mg or placebo. After a mean follow-up of 39.8 months, the primary composite of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke occurred in 6.5 percent of the semaglutide arm and 8.0 percent of the placebo arm. Hazard ratio 0.80, 95 percent confidence interval 0.72 to 0.90, P less than 0.001 (Lincoff et al., NEJM 2023, PMID 37952131). That readout, on March 8 2024, gave Wegovy its FDA cardiovascular indication.
The interesting question is not whether the 20 percent reduction is real. It is what is doing the work. Five prespecified secondary analyses have now read out, and the picture they paint is that most of the cardiovascular benefit is not the weight loss.
What SELECT actually enrolled
The eligibility criteria matter for how far the result generalizes.
| Inclusion | Specifics |
|---|---|
| Age | 45 years or older |
| BMI | 27 kg/m² or higher |
| Cardiovascular history | Prior MI, prior stroke, or symptomatic peripheral artery disease |
| Diabetes status | No diabetes diagnosis; HbA1c below 6.5% |
| Optimal medical therapy | Required (statins, antiplatelets, RAAS blockade where indicated) |
Mean baseline age was 61.6 years, 72.3 percent male, mean BMI 33.4. Baseline HbA1c was below 5.7 percent in 33.5 percent of participants, 5.7 to under 6.0 percent in 34.6 percent, and 6.0 to under 6.5 percent in 31.9 percent (Lingvay et al., Diabetes Care 2024, PMID 38907684). That distribution matters because the treatment effect held in all three HbA1c strata, including the under-5.7 percent group where no one was anywhere near a diabetes diagnosis. The benefit cannot be explained away as treatment of subclinical diabetes.
What SELECT did not enroll: people under 45, people with diabetes, people with NYHA class IV heart failure, people with prior medullary thyroid carcinoma or MEN2, and people without established atherosclerotic disease. The trial does not tell you what semaglutide does in primary prevention populations.
The primary endpoint and its decomposition
The headline composite breaks down across the three components and the major secondaries.
| Endpoint | Semaglutide (n=8,803) | Placebo (n=8,801) | Hazard ratio (95% CI) |
|---|---|---|---|
| MACE (primary) | 569 (6.5%) | 701 (8.0%) | 0.80 (0.72 to 0.90) |
| Nonfatal MI | 234 (2.7%) | 322 (3.7%) | 0.72 (0.61 to 0.85) |
| CV death | 223 (2.5%) | 262 (3.0%) | 0.85 (0.71 to 1.01) |
| Nonfatal stroke | 153 (1.7%) | 154 (1.7%) | 0.99 (0.79 to 1.24) |
| All-cause death | 375 (4.3%) | 414 (4.7%) | 0.81 (0.71 to 0.93) |
All numbers from Lincoff et al., NEJM 2023, PMID 37952131. The MI signal is doing most of the work in the composite. The stroke arm sits at unity. CV death moves but does not reach conventional significance on its own; the all-cause mortality reduction does.
Bottom line: SELECT is a real positive trial driven mostly by reductions in nonfatal myocardial infarction, with a supportive but less precise signal on cardiovascular and all-cause death and no separation on stroke.
The weight-mediation question
The default assumption in 2024 was that the cardiovascular benefit was the weight loss. The 2025 mediation analysis from John Deanfield's group complicated that story.
Deanfield et al., Lancet 2025, PMID 41138739 ran the prespecified adiposity analysis. Three findings stand out. First, the cardiovascular benefit was consistent across baseline body weight, BMI, and waist circumference categories. Second, the magnitude of early weight loss at 20 weeks did not predict subsequent MACE risk in the semaglutide arm. Third, changes in waist circumference were associated with MACE, but a mediation analysis estimated that only about 33 percent of the observed treatment effect was mediated through waist-circumference change.
That is the inversion: roughly two thirds of the MACE benefit is not explained by the adiposity reduction that semaglutide produces. The mechanistic candidates that fit that pattern include direct anti-inflammatory effects, plaque-stabilization signals, blood-pressure reduction independent of weight, and changes in atherogenic lipid handling. None of those are individually proven in SELECT. What SELECT establishes is that the weight-loss story is incomplete.
For background on the lean-mass cost that accompanies the weight loss, and why body composition matters separately from total weight, see GLP-1 muscle loss research.
The heart failure subgroup is bigger, not smaller
A common worry going into SELECT was that heart failure patients, especially those with reduced ejection fraction, might do worse on a GLP-1 receptor agonist. The opposite happened.
Deanfield et al., Lancet 2024, PMID 39181597 ran the prespecified heart failure analysis. Of the 17,604 enrolled, 4,286 (24.3 percent) had a history of investigator-defined heart failure: 53.0 percent HFpEF, 31.4 percent HFrEF, 15.5 percent unclassified. In the heart failure cohort, MACE hazard ratio was 0.72 (95 percent CI 0.60 to 0.87). The heart failure composite (cardiovascular death plus hospitalization or urgent visit for heart failure) had a hazard ratio of 0.79 (0.64 to 0.98). The treatment effect was directionally consistent across HFpEF and HFrEF subtypes.
The pooled heart-failure analysis across SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM (Kosiborod et al., Lancet 2024, PMID 39222642) sharpened the HFpEF signal. The combined endpoint of cardiovascular death or worsening heart failure events was 5.4 percent on semaglutide versus 7.5 percent on placebo (HR 0.69, 95 percent CI 0.53 to 0.89). Worsening heart failure alone dropped from 4.7 percent to 2.8 percent (HR 0.59, 95 percent CI 0.41 to 0.82).
For comparison with tirzepatide in a dedicated HFpEF trial, see the SUMMIT trial evidence in tirzepatide HFpEF.
Kidney outcomes look like a separate signal
Colhoun et al., Nature Medicine 2024, PMID 38796653 reported the prespecified kidney composite. The endpoint combined persistent eGFR reduction of 50 percent or more, persistent eGFR below 15, kidney replacement therapy, kidney death, and persistent macroalbuminuria. Incidence was 1.8 percent on semaglutide and 2.2 percent on placebo, hazard ratio 0.78 (95 percent CI 0.63 to 0.96, P=0.02). The eGFR treatment effect at 104 weeks was a modest 0.75 mL/min/1.73 m² overall, rising to 2.19 mL/min/1.73 m² in patients with a baseline eGFR below 60.
This is a smaller absolute effect than SELECT showed on cardiovascular outcomes, but it points in the same direction and is consistent with what the dedicated kidney trial showed in diabetic CKD. See semaglutide FLOW trial in CKD evidence for the FLOW-specific readout.
Long-term weight loss in non-diabetics
Ryan et al., Nature Medicine 2024, PMID 38740993 extended the weight curve out to 208 weeks. Mean body-weight reduction was 10.2 percent on semaglutide versus 1.5 percent on placebo at four years. Waist circumference dropped 7.7 cm vs 1.3 cm. Weight loss continued through approximately week 65 and was sustained thereafter. Serious adverse events were lower on semaglutide than placebo (33.4 percent vs 36.8 percent), which is the inverse of the pattern you usually see in long-duration obesity-drug trials.
The lower SAE rate is largely driven by reductions in cardiovascular and metabolic adjudicated events. The headline tolerability problem, gastrointestinal side effects, was higher on semaglutide and drove most of the differential discontinuation: study-drug discontinuation due to adverse events was about 16.6 percent on semaglutide vs 8.2 percent on placebo in the primary trial. The nausea/vomiting profile is what most patients drop out for, not what hurts them long-term.
For the practical mechanics of weekly subcutaneous semaglutide and the dose-titration ladder, see the semaglutide reconstitution chart and the Wegovy HD 7.2 mg STEP UP guide for the next dose tier above the SELECT regimen.
Who SELECT actually applies to
A decision matrix is the cleanest way to read the trial out:
| Patient profile | SELECT applies | Notes |
|---|---|---|
| Adult 45+, established CVD, BMI 27+, no diabetes | Yes, directly | This is the enrolled population |
| Adult with established CVD plus diabetes | Use SUSTAIN-6 and FLOW, not SELECT | SELECT excluded diabetes |
| Younger adult, obesity, no CVD | Out of scope | Trial enrolled only 45+ with prior CV event |
| HFpEF with obesity, no diabetes | Supported by SELECT HF subgroup + STEP-HFpEF | Effect size larger than overall trial |
| HFrEF with obesity, no diabetes | Supported by SELECT HF subgroup | Smaller numerical subgroup but consistent direction |
| Stroke prevention as the primary goal | Not supported | Stroke component of MACE sat at unity |
| Severe CKD (eGFR under 30) | Limited applicability | SELECT did not enroll dialysis or near-dialysis patients |
Warning: SELECT does not establish that semaglutide prevents heart attacks in low-risk primary-prevention populations. The trial enrolled only adults with prior MI, stroke, or symptomatic PAD. Extending the result to people without established disease is an inference the data do not directly support.
Where this sits in the broader semaglutide evidence map
SELECT is the cardiovascular pillar of a four-pillar Phase 3 program that also includes FLOW (CKD with diabetes), STEP-HFpEF (HFpEF with obesity), and ESSENCE (MASH). For the liver-disease readout, see semaglutide ESSENCE Phase 3 in MASH. For knee osteoarthritis, where the same compound at the same dose produced a smaller but real pain-and-function benefit, see STEP 9 in knee osteoarthritis. For the muscle-mass tradeoff that applies across every GLP-1 trial including SELECT, see GLP-1 lean mass research.
The unifying observation across these readouts is that semaglutide produces benefits in tissue beds (kidney, heart, liver, joints) at a magnitude that is not proportional to the weight loss in any of them. SELECT was the first trial to formally show that pattern with a mediation analysis.
For where this sits versus the head-to-head GIP/GLP-1 co-agonist program, the GLP-1 dosing comparison 2026 covers semaglutide alongside tirzepatide, retatrutide, and orforglipron, and tirzepatide HFpEF SUMMIT evidence covers the analogous cardiometabolic readout for the GIP/GLP-1 co-agonist.
Practical sourcing
The compound used in SELECT was Novo Nordisk's branded semaglutide. The FDA-approved formulations for cardiovascular risk reduction (Wegovy 2.4 mg) and type 2 diabetes (Ozempic) are available only through traditional retail pharmacies on prescription.
Research-grade semaglutide for non-clinical use is available from Ascension Peptides with 50% off using code ENHANCED. For reconstitution math and dosing volumes that match the SELECT regimen, the reconstitution calculator handles unit conversion across syringe sizes.
The honest evidence summary
SELECT is the strongest cardiovascular outcomes trial in the obesity-without-diabetes population that has ever been run. The 20 percent MACE reduction is real, the direction is consistent across MI, CV death, and all-cause death, and the heart-failure and kidney subgroup analyses point the same way. The weight-mediation story is more complicated than it looked in 2024: roughly two thirds of the cardiovascular benefit is not explained by the adiposity change semaglutide produces.
What the trial does not establish: a benefit in primary prevention, a benefit in people with diabetes (use SUSTAIN-6 and FLOW for those populations), a benefit on stroke specifically, or a clean mechanistic explanation for the residual weight-independent effect. Those questions are open and active in 2026.
References
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. PMID 37952131
- Ryan DH, Lingvay I, Deanfield J, et al. Long-term weight loss effects of semaglutide in obesity without diabetes in the SELECT trial. Nat Med. 2024;30(7):2049-2057. PMID 38740993
- Colhoun HM, Lingvay I, Brown PM, et al. Long-term kidney outcomes of semaglutide in obesity and cardiovascular disease in the SELECT trial. Nat Med. 2024;30(7):2058-2066. PMID 38796653
- Deanfield J, Verma S, Scirica BM, et al. Semaglutide and cardiovascular outcomes in patients with obesity and prevalent heart failure: a prespecified analysis of the SELECT trial. Lancet. 2024;404(10454):773-786. PMID 39181597
- Kosiborod MN, Petrie MC, Borlaug BA, et al. Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM randomised trials. Lancet. 2024;404(10456):949-961. PMID 39222642
- Lingvay I, Deanfield J, Kahn SE, et al. Semaglutide and Cardiovascular Outcomes by Baseline HbA1c and Change in HbA1c in People With Overweight or Obesity but Without Diabetes in SELECT. Diabetes Care. 2024;47(8):1360-1369. PMID 38907684
- Deanfield J, Lingvay I, Ryan DH, et al. Semaglutide and cardiovascular outcomes by baseline and changes in adiposity measurements: a prespecified analysis of the SELECT trial. Lancet. 2025. PMID 41138739
This article is for educational and research purposes only. None of the content above constitutes medical advice. Semaglutide is FDA approved as Ozempic for type 2 diabetes, as Wegovy for chronic weight management and for cardiovascular risk reduction in adults with established cardiovascular disease and overweight or obesity, and as Rybelsus for type 2 diabetes. Doses, regimens, and trial summaries described here describe what the published literature tested under controlled conditions; they are not protocols and do not establish efficacy or safety for any specific individual. Decisions about cardiovascular prevention and obesity pharmacotherapy belong with the patient and a qualified clinician.