At a glance
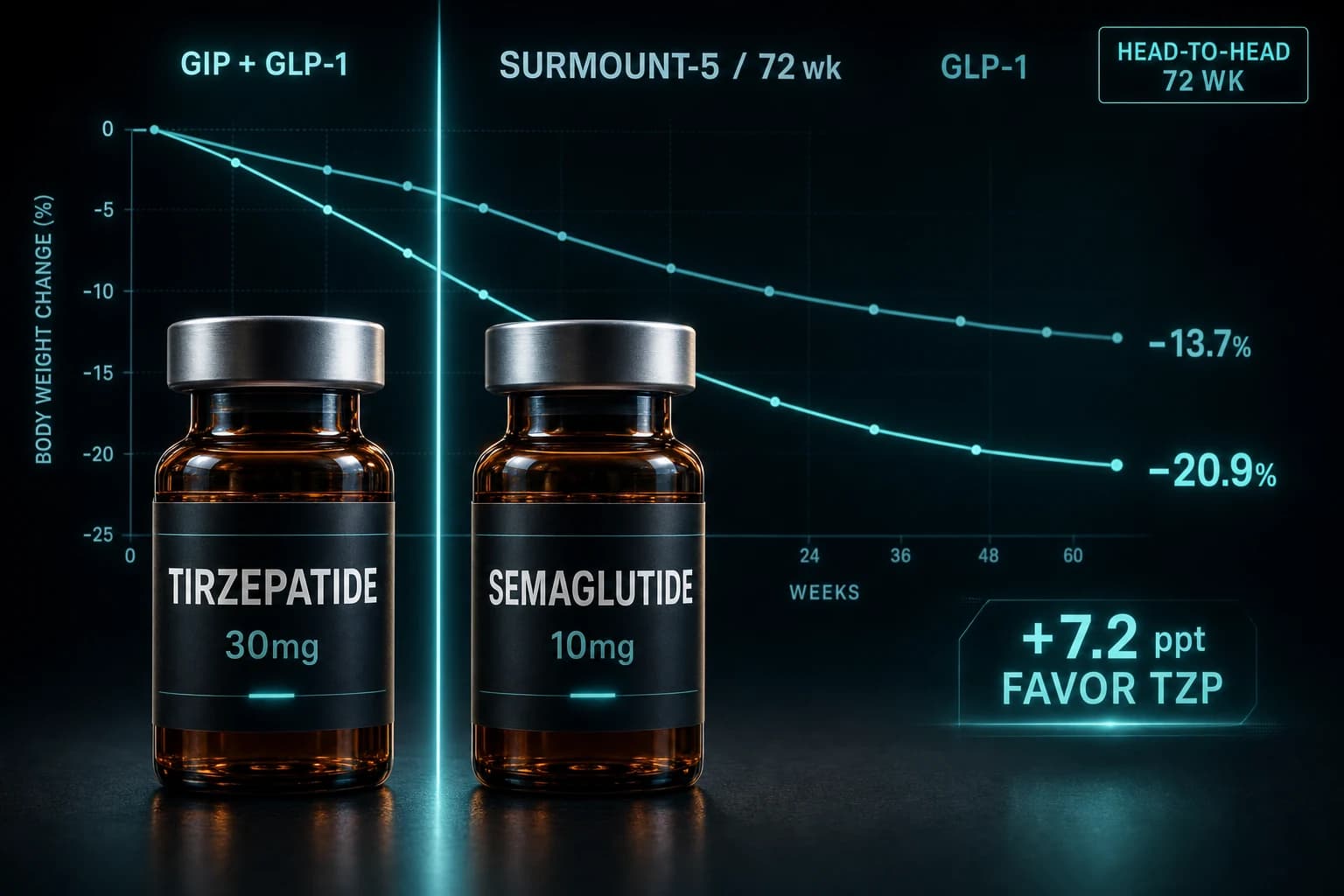
- SURMOUNT-5 (Aronne 2025, NEJM): 751 adults, MTD tirzepatide vs MTD semaglutide, 72 weeks
- Mean body weight change: -20.2% on tirzepatide vs -13.7% on semaglutide at week 72
- ≥15% weight loss reached by 64.6% on tirzepatide vs 40.1% on semaglutide
- ≥30% weight loss reached by 19.7% vs 6.9%; the gap widens at the upper response tail
- GI-driven discontinuation was lower on tirzepatide (2.7% vs 5.6%): no tolerability penalty for the dual agonist
A real head to head finally exists
Until May 2025, the case for tirzepatide over semaglutide rested on indirect comparisons and one trial in diabetes patients. Obesity-only readers had nothing definitive: cross-trial weight numbers from SURMOUNT-1 and STEP 1 that the field treated as roughly comparable. SURMOUNT-5 changes that read. Eli Lilly funded the trial, randomized 751 adults with obesity but without type 2 diabetes 1:1 to tirzepatide or semaglutide at maximum tolerated doses, ran it 72 weeks, and reported what is now the cleanest peer-reviewed comparison of the two drugs (Aronne et al. NEJM 2025, PMID 40353578).
The headline: tirzepatide produced 20.2% body weight reduction vs 13.7% on semaglutide at week 72. That is a 6.5 percentage point gap at the same endpoint, with the same lifestyle program, in patients with the same baseline characteristics. The result holds across published subgroup analyses and responder thresholds, not just in the average.
Bottom line: SURMOUNT-5 is the first published, peer-reviewed, head-to-head obesity trial of tirzepatide versus semaglutide at maximum tolerated doses. Tirzepatide produced 6.5 percentage points more weight loss at 72 weeks, fewer treatment-limiting GI adverse events, and a larger predicted 10-year cardiovascular risk reduction. Open-label design and the MTD vs MTD comparison (instead of fixed 15 mg vs 2.4 mg) are the main caveats.
What SURMOUNT-5 actually tested
SURMOUNT-5 is a Phase 3b open-label controlled trial. The open-label design matters for interpretation. Both patients and clinicians knew which drug each participant received. Subjective endpoints (reported tolerability, quality of life) are more vulnerable to expectancy effects in this design than they would be in a double-blind comparison. Objective endpoints (body weight, waist, lab values) are not.
Trial design at a glance:
| Feature | SURMOUNT-5 |
|---|---|
| Phase | 3b |
| Blinding | Open-label |
| Participants | 751 adults |
| Randomization | 1:1, tirzepatide vs semaglutide |
| Tirzepatide dose | MTD: 10 mg or 15 mg weekly |
| Semaglutide dose | MTD: 1.7 mg or 2.4 mg weekly |
| Treatment duration | 72 weeks |
| Population | Obesity without type 2 diabetes |
| Mean baseline age | 44.7 years |
| Female participants | 64.7% |
| Lifestyle program | Diet plus exercise counseling, both arms |
Two design choices shape how you read the result. First, this was maximum-tolerated dose vs maximum-tolerated dose. Both arms titrated to the highest dose each patient could tolerate, with the lower options (10 mg tirzepatide, 1.7 mg semaglutide) available as the ceiling for participants who could not stay on the top dose. That mirrors real-world prescribing. It does not mirror a head-to-head at the fully labeled top dose (15 mg versus 2.4 mg), which would have widened the gap further toward tirzepatide. Second, the 72-week duration matches the time horizon of SURMOUNT-1 and STEP 1, which keeps the SURMOUNT-5 numbers directly comparable to the foundational obesity trials of each drug.
The headline result, expanded
Trial endpoints at week 72, least-squares mean changes from baseline:
| Endpoint | Tirzepatide MTD | Semaglutide MTD | Gap |
|---|---|---|---|
| Mean body weight change | -20.2% | -13.7% | -6.5 percentage points |
| Mean absolute weight loss | -22.8 kg | -15.0 kg | -7.8 kg |
| Waist circumference change | -18.4 cm | -13.0 cm | -5.4 cm |
| Reached ≥15% loss | 64.6% | 40.1% | +24.5 percentage points |
| Reached ≥25% loss | 31.0% | 16.1% | +14.9 percentage points |
| Reached ≥30% loss | 19.7% | 6.9% | +12.8 percentage points |
| 10-year predicted CVD risk reduction | -23.7% | -13.6% | -10.1 percentage points |
| GI-driven discontinuation | 2.7% | 5.6% | -2.9 percentage points |
Sources: primary trial paper (PMID 40353578) and the post-hoc cardiovascular risk analysis (PMID 40980721).
The 6.5 percentage point gap in mean weight loss tracks what indirect comparisons across SURMOUNT-1 and STEP 1 had been suggesting since 2022. SURMOUNT-1 reported 20.9% mean weight loss on tirzepatide 15 mg in 2,539 adults with obesity over 72 weeks (Jastreboff et al. NEJM 2022, PMID 35658024). STEP 1 reported 14.9% on semaglutide 2.4 mg in 1,961 adults over 68 weeks (Wilding et al. NEJM 2021, PMID 33567185). SURMOUNT-5 confirms the cross-trial gap is not an artifact of patient selection.
Where the gap is biggest
The 20.2-versus-13.7 comparison flattens a non-uniform difference. The gap widens at the high end of the weight loss distribution. Look at the responder thresholds: the ≥15% threshold favored tirzepatide by 24.5 percentage points, the ≥25% threshold by 14.9 points, and the ≥30% threshold by 12.8 points. Roughly one in five people on tirzepatide MTD lost 30% or more of their body weight. On semaglutide MTD, that number was closer to one in fifteen.
Clinical interpretation: the average gap is real, but most of it lives in the upper response tail. Both drugs are effective for the moderate responder who lands somewhere between 5 and 15% loss. They diverge sharply in the population that, for reasons not fully understood, responds aggressively to incretin therapy.
Sex was a meaningful subgroup. Women lost more weight than men in both arms, with a similar relative gap between drugs in each sex. That pattern reverses the typical lifestyle-only result, where men usually outpace women on absolute weight loss in early months. The mechanism is not characterized, but it is consistent across SURMOUNT and STEP trial families.
Tolerability: the gap that surprised people
Going into SURMOUNT-5, the assumption among many prescribers was that tirzepatide's larger weight loss would come at a tolerability cost. The trial does not support that. GI-driven discontinuation was 2.7% on tirzepatide versus 5.6% on semaglutide. Treatment-related GI events (nausea, diarrhea, constipation, vomiting) were common in both arms, as expected for any incretin agent, but they were more likely to drive a patient off semaglutide than off tirzepatide.
That pattern matches SURPASS-2, the first head-to-head of these two drugs, run in type 2 diabetes, which reported similar GI tolerability with a directional edge toward tirzepatide (Frias et al. NEJM 2021, PMID 34170647). SURMOUNT-5 extends the pattern outside diabetes. The dual GIP/GLP-1 mechanism does not appear to carry a meaningful tolerability penalty over pure GLP-1 agonism at maximum tolerated doses.
Tip: If a previous semaglutide attempt failed because of nausea, the SURMOUNT-5 tolerability profile does not predict a worse experience on tirzepatide. The reverse may be true, although the head-to-head was not powered to test sequential switching.
Cardiovascular risk and quality of life
The post-hoc cardiovascular analysis is one of the more interesting reads from the trial. Predicted 10-year CVD risk fell 23.7% on tirzepatide versus 13.6% on semaglutide (PMID 40980721). Absolute reduction from baseline was 2.4 versus 1.4 percentage points, p<0.001. That gap is driven by the larger weight, waist, and metabolic-marker improvements on tirzepatide. It is not the same as a direct major adverse cardiovascular event (MACE) trial. Hard cardiovascular endpoint data for semaglutide already exists from SELECT: a 20% reduction in MACE in 17,604 adults with obesity and prior CVD (Lincoff et al. NEJM 2023, PMID 37952131). Tirzepatide's dedicated cardiovascular outcomes trial (SURPASS-CVOT) has reported topline but not yet published a peer-reviewed primary readout.
Quality of life improved with both drugs at week 72. SF-36v2 physical-component scores rose significantly in both arms, mental-component scores were flat in both arms, and the General Health domain improved more with tirzepatide (5.45 versus 4.20, p=0.003) (PMID 41187971). The mental health no-change result is worth flagging: weight loss in these trials does not automatically translate to subjective mental health improvement, even when participants are losing 15 to 20% of their body weight.
What SURMOUNT-5 does not answer
The trial is the strongest comparison evidence to date, but several questions sit outside its scope:
- Fixed top dose vs fixed top dose. SURMOUNT-5 used MTD, not labeled top doses. A 15 mg vs 2.4 mg comparison would likely show a larger gap, but no such trial has been published.
- Long-term durability beyond 72 weeks. Both drugs require continued dosing to maintain weight loss. The STEP 4 and SURMOUNT-4 withdrawal designs have shown regain on discontinuation. The withdrawal evidence breakdown is the cleanest read on what happens when you stop.
- Effect in real-world adherence settings. Trial adherence is higher than community adherence. Retrospective US cohort studies show a smaller but still significant tirzepatide advantage in actual practice.
- Body composition partitioning. SURMOUNT-5 measured weight and waist, not DXA-quantified lean versus fat mass. Lean mass preservation is one of the open questions for the entire incretin class. The GLP-1 muscle loss research breakdown summarizes what the existing evidence says.
- Higher-dose semaglutide. Wegovy HD at 7.2 mg weekly is now approved on the STEP UP trial data. SURMOUNT-5 used the 2.4 mg max. A 7.2 mg arm would change the comparison; the Wegovy HD 7.2 mg trial guide covers what that dose actually showed.
How to read this if you are choosing between them
For a person comparing the two drugs purely on weight loss potential, SURMOUNT-5 provides a defensible answer: tirzepatide is the more effective option at MTD in adults with obesity and no diabetes. The gap is meaningful at the average, larger at the response tail, and not paid for by worse GI tolerability. The cardiovascular signal directionally favors tirzepatide on predicted risk, although semaglutide owns the only published MACE outcome data so far.
That said, the choice is not as binary as the trial result reads. Semaglutide reaches lower starting doses, has a longer real-world track record, and now has the higher-dose 7.2 mg option that did not exist in SURMOUNT-5. Tirzepatide's larger gap shows up most clearly in patients aiming for greater than 20% body weight loss. For a moderate target (5 to 10%), both drugs comfortably reach the goal in the majority of responders.
Research-use audience notes: both molecules are widely available through compounding pharmacies and the research peptide market in 2026. Reconstitution math is non-trivial for both. The reconstitution calculator handles the IU conversions for any vial size. Compound-specific guides for tirzepatide and semaglutide cover dose ranges, half-life, and stability behavior. The cross-class GLP-1 dosing comparison puts SURMOUNT-5 alongside the dose ladders for retatrutide, orforglipron, and Wegovy HD.
For research-grade injectables that ship with verifiable certificates of analysis, Ascension Peptides carries both tirzepatide and semaglutide; code ENHANCED takes 50 percent off. Oral semaglutide and adjacent oral formats are available from Limitless Biotech; code ENHANCED applies.
Warning: SURMOUNT-5 measured outcomes under direct clinical supervision with diet and exercise counseling. The published response curves do not translate cleanly to self-directed use without that supervision. Trial conditions are not the same as research-use conditions.
What this means for the broader GLP-1 field
SURMOUNT-5 has implications beyond the tirzepatide-versus-semaglutide question. The trial validates the mechanistic thesis that GIP agonism on top of GLP-1 agonism adds meaningful weight loss, rather than just acting as a tolerability buffer. That has direct implications for the next generation of incretin drugs. Retatrutide (GLP-1 plus GIP plus glucagon triple agonist) builds on the same logic. Maridebart cafraglutide (MariTide), which antagonizes GIP rather than activating it, will need to show that it can match or beat semaglutide alone in a fair head-to-head before the field abandons the GIP-agonism thesis.
Higher-dose semaglutide and the SELECT CVOT data remain the strongest counter-arguments for keeping semaglutide as a first-line GLP-1 in many practice settings. The semaglutide SELECT MACE evidence breakdown is the most consequential cardiovascular data set the field has on any incretin. Tirzepatide will need its own published MACE readout before the CV question is fully settled.
For an evidence-based prescriber or researcher, the practical implication is straightforward. Tirzepatide is the more potent weight loss agent at MTD. Semaglutide is the agent with the most cardiovascular outcome evidence. Both are real, both are useful, and the choice depends on the specific clinical or research target.
References
- Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. N Engl J Med. 2025;393:26-36. PMID 40353578
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387:205-216. PMID 35658024
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384:989-1002. PMID 33567185
- Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385:503-515. PMID 34170647
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389:2221-2232. PMID 37952131
- Tirzepatide compared with semaglutide and 10-year cardiovascular disease risk reduction in obesity: post-hoc analysis of the SURMOUNT-5 trial. Eur Heart J Open. 2025. PMID 40980721
- Improved health-related quality of life with tirzepatide versus semaglutide in adults with obesity or overweight from the SURMOUNT-5 trial. Diabetes Obes Metab. 2026. PMID 41187971
This article is for educational and research purposes only. None of the content above constitutes medical advice. Tirzepatide and semaglutide are prescription drugs in the United States and most jurisdictions; research-use peptide markets operate under separate disclosures and are not authorized for human consumption. The numbers above describe what published clinical trials measured under supervised conditions. They do not establish efficacy or safety for any specific individual. Decisions about weight management or any medical use of these compounds belong with the patient and a qualified clinician.