At a glance
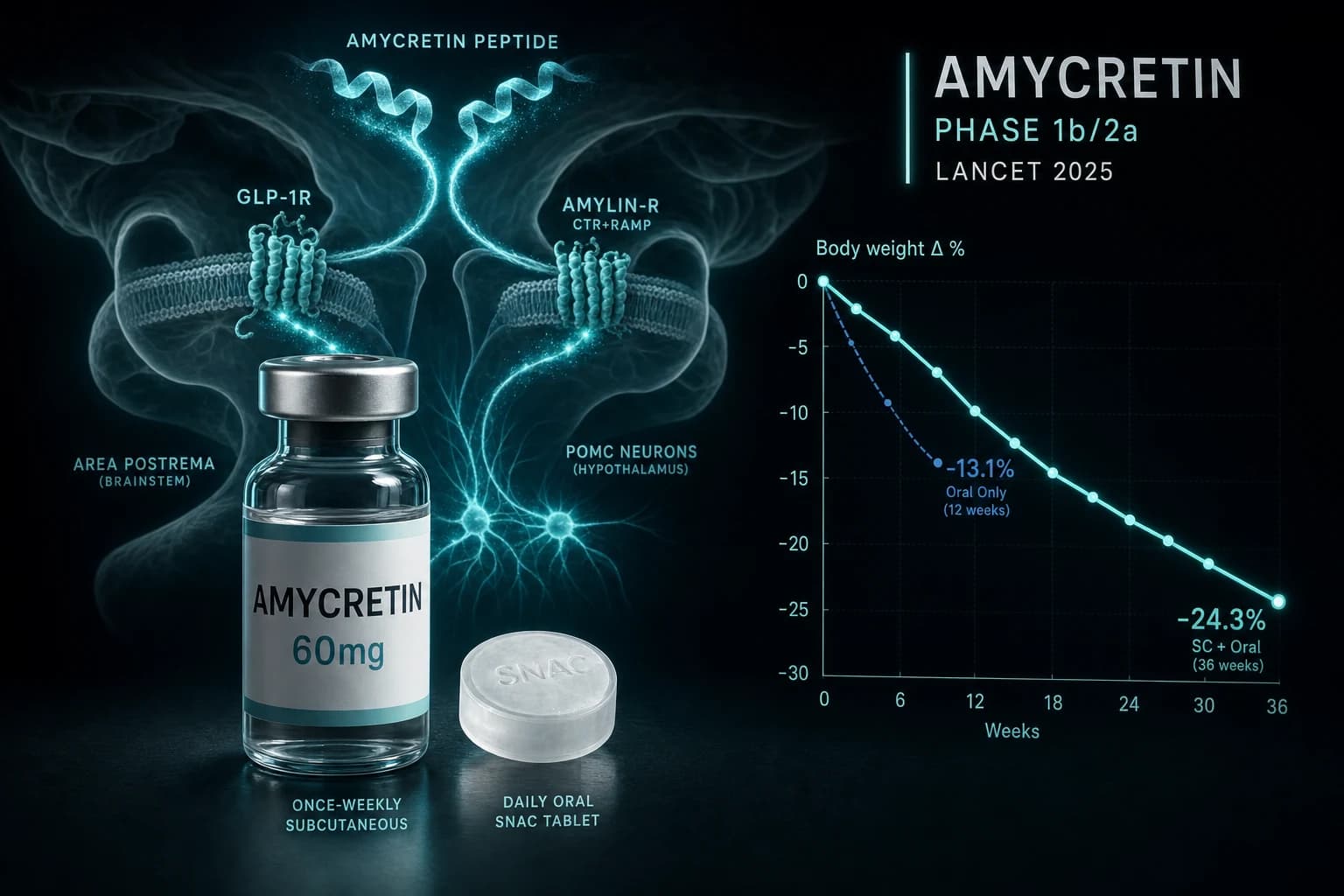
- Subcutaneous amycretin Phase 1b/2a (Lancet 2025, PMID 40550231): -24.3% mean weight change at 36 weeks on the 60 mg dose escalation arm vs -1.1% placebo in 125 adults with overweight or obesity
- Oral amycretin Phase 1 (Lancet 2025, PMID 40550229): -13.1% mean weight change at 12 weeks on 50 mg twice daily vs -1.2% placebo in 144 adults
- First peptide to combine GLP-1 receptor agonism and amylin receptor agonism in a single molecule; developed in parallel as once-weekly subcutaneous and once-daily oral formulations
- Novo Nordisk opened Phase 3 obesity enrollment in Q1 2026; no head-to-head versus active comparators, no cardiovascular outcome trial, no MASH biopsy data yet
- Weight loss did not plateau at any subcutaneous dose by end of treatment, suggesting longer durations may produce additional reduction; the Phase 1 trials cannot quantify how much
Why amycretin matters for the obesity drug pipeline
Once-weekly subcutaneous amycretin produced a mean body weight reduction of 24.3 percent at 36 weeks in the highest dose arm of its first-in-human trial, compared with 1.1 percent on placebo (Lancet 2025, PMID 40550231). The oral version, dosed twice daily, hit 13.1 percent at 12 weeks versus 1.2 percent on placebo (Lancet 2025, PMID 40550229). Novo Nordisk published both data sets on the same day in June 2025 and opened Phase 3 obesity enrollment in the first quarter of 2026.
That is the headline. Read carefully, the trials were small, short, and not designed to compare amycretin against an active drug. The 24.3 percent figure came from a dose escalation arm, not a steady state maintenance period. Everything in this article is built on Phase 1 evidence in fewer than 300 humans. Treat the numbers below as proof of concept, not the read on what amycretin will produce in a registrational trial.
Bottom line: Amycretin is the first molecule to combine GLP-1 and amylin receptor activity in a single drug substance. Phase 1 evidence is competitive with the strongest existing obesity drugs. Phase 3 readouts will not arrive for at least two years, and there is no clinical availability today.
What amycretin is, molecularly
Amycretin is a long-acting, unimolecular peptide that activates two distinct receptors: the GLP-1 receptor (GLP-1R) and the amylin receptor, which is the calcitonin receptor complexed with a receptor activity modifying protein (RAMP1 or RAMP3). Both receptor families sit in brainstem and hypothalamic circuits that govern appetite, gastric emptying, and meal termination. A single peptide acting on both at engineered ratios is the first time the obesity field has tested GLP-1 and amylin biology delivered through one drug substance in humans.
Two formulations are being developed in parallel. The subcutaneous version is dosed once weekly with a fatty acid linker that anchors the peptide to circulating albumin and stretches the half-life to support weekly administration. The oral version is dosed once daily and uses the SNAC enabling agent (sodium N-(8-[2-hydroxybenzoyl] amino) caprylate), the same buccal absorption technology that makes oral semaglutide (Rybelsus) viable in a pill. Both formulations finished Phase 1 in 2025 and both are headed into Phase 3 obesity programs starting in the first quarter of 2026.
For context on the GLP-1 half of the molecule, see the semaglutide compound profile. For the amylin half, see the cagrilintide compound profile.
Why amylin matters alongside GLP-1
Amylin is a 37 amino acid peptide co-secreted with insulin from pancreatic beta cells after a meal. In the brain, amylin receptors concentrate in the area postrema and the nucleus of the solitary tract, two brainstem structures that share circuitry with central GLP-1 signaling. Amylin slows gastric emptying, suppresses postprandial glucagon, and activates POMC neurons in the hypothalamic arcuate nucleus, three effects that converge on satiety and meal termination (Walker et al., Nature Reviews Endocrinology 2025, PMID 40360789).
Clinical interest in combining the two pathways predates amycretin. Pramlintide (Symlin), an early amylin analogue, was FDA approved as an adjunct to mealtime insulin in type 1 and type 2 diabetes in 2005. Pramlintide reduced energy intake by 23 percent in adults with type 2 diabetes and 16 percent in obese subjects without diabetes in a controlled feeding study (Lancet 2005, PMID 15843914). Cagrilintide, a long acting amylin analogue dosed weekly, hit 10.8 percent mean weight loss versus 3.0 percent on placebo at 26 weeks in a Phase 2 dose finding trial (Lau et al., Lancet 2021, PMID 34798060).
Combining cagrilintide and semaglutide (CagriSema) in a single weekly injection is the closest existing analogue of what amycretin tries to do in one peptide. CagriSema produced 20.4 percent mean weight loss at 68 weeks in the REDEFINE 1 Phase 3 trial, compared with 14.9 percent on semaglutide alone and 11.5 percent on cagrilintide alone (NEJM 2025, DOI 10.1056/NEJMoa2502081). Two drugs in one injection added roughly 5 to 9 percentage points over either drug alone. That separation is the clinical signal that motivated the amycretin program.
Animal models supply the mechanistic basis. In rodents, dual GLP-1 plus amylin receptor activation produced larger reductions in food intake and body weight than either pathway alone. The amylin half of the effect depended on amylin receptor 1 and 3 subtypes; knockouts blunted weight loss. Amycretin is testing whether one molecule can do what two molecules already do, with cleaner pharmacokinetics and simpler patient adherence.
Subcutaneous amycretin: Phase 1b/2a in 125 adults
The subcutaneous trial enrolled 125 adults with overweight or obesity at a single research site in San Antonio, Texas. Participants were randomized across single ascending dose, multiple ascending dose, and dose response arms, with maintenance dosing periods ranging from 20 to 36 weeks. The trial was not designed to compare doses against each other, and the highest dose arm reached 60 mg through escalation rather than a fixed maintenance phase. With those caveats, the published body weight data (Lancet 2025, PMID 40550231) lined up as follows:
| Subcutaneous arm | Top maintenance dose | Treatment duration | Mean weight change | Placebo arm |
|---|---|---|---|---|
| Part B | 60 mg (escalation) | 36 weeks | -24.3% | -1.1% |
| Part C | 20 mg | 36 weeks | -22.0% | +1.9% |
| Part D | 5 mg | 28 weeks | -16.2% | +2.3% |
| Part E | 1.25 mg | 20 weeks | -9.7% | +2.0% |
A 24.3 percent figure is doing a lot of work in press headlines. Read carefully, it came from a dose escalation arm where 60 mg was the endpoint of an up-titration, not a steady state maintenance dose held for the entire 36 weeks. The 20 mg maintenance arm is the cleaner number for comparison at 22.0 percent at the same 36 week endpoint. Both figures exceeded what semaglutide and tirzepatide produced at comparable timepoints in their own early studies, but neither was tested against an active comparator inside the same trial.
One other observation is worth flagging: body weight did not plateau by the end of treatment in any arm. The trial authors said as much directly. Phase 3 will run longer than 36 weeks and the expectation is that more weight loss is possible. The Phase 1 data cannot quantify how much more.
Oral amycretin: Phase 1 in 144 adults
The oral trial enrolled 144 adults across single ascending dose and multiple ascending dose parts, with treatment up to 12 weeks (Lancet 2025, PMID 40550229). The maintenance arms most often quoted used 50 mg once daily and 50 mg twice daily (100 mg total daily exposure). Results at 12 weeks:
| Oral arm | Total daily dose | Treatment duration | Mean weight change | Placebo arm |
|---|---|---|---|---|
| Multiple ascending, low | 50 mg once daily | 12 weeks | -10.4% | -1.2% |
| Multiple ascending, high | 50 mg twice daily | 12 weeks | -13.1% | -1.2% |
Oral amycretin uses the SNAC enabling agent, the same buccal absorption technology that allows oral semaglutide (Rybelsus) to clear stomach acid intact. Bioavailability is low, the doses are correspondingly high (50 mg twice daily versus 14 mg for top dose Rybelsus), and dosing instructions require a fast on either side of the tablet to maximize absorption. The general absorption constraints of orally bioavailable peptides apply. For more on the format difference, see the injectable vs oral peptides bioavailability guide.
What the oral data show is that amycretin is the first dual receptor obesity drug being developed as a true oral pill. Tirzepatide, cagrilintide, retatrutide, mazdutide, and survodutide are all injectable. Orforglipron is the leading oral monoagonist GLP-1 in Phase 3 development. Amycretin is the first oral candidate to pair GLP-1 with a second mechanism in a single tablet.
Where amycretin sits next to the rest of the class
Cross-trial comparisons are unreliable because populations, durations, dose schedules, and lifestyle interventions all differ. The table below pulls the cleanest published numbers from each program for context, not for ranking.
| Drug | Mechanism | Trial / Phase | Top mean weight change | Duration |
|---|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 mono | STEP 1 (Phase 3) | -14.9% | 68 weeks |
| Tirzepatide 15 mg | GIP / GLP-1 dual | SURMOUNT-1 (Phase 3) | -20.9% | 72 weeks |
| Retatrutide 12 mg | GIP / GLP-1 / glucagon triple | Phase 2 obesity | -24.2% | 48 weeks |
| Cagrilintide 4.5 mg | Amylin mono | Phase 2 dose finding | -10.8% | 26 weeks |
| CagriSema 2.4/2.4 mg | Amylin + GLP-1 (two molecules) | REDEFINE 1 (Phase 3) | -20.4% (ITT) / -22.7% (adherent) | 68 weeks |
| Amycretin SC 60 mg (escalation) | GLP-1 / amylin dual (one molecule) | Phase 1b/2a | -24.3% | 36 weeks |
| Amycretin oral 100 mg/day | GLP-1 / amylin dual (one molecule) | Phase 1 | -13.1% | 12 weeks |
The amycretin number sits in the same range as retatrutide and ahead of single mechanism GLP-1s. The honest read is that 36 weeks is short and 125 participants is small. None of the older drugs above produced their peak in Phase 1. Several lost a few percentage points moving from Phase 2 to Phase 3 once larger and more diverse populations entered the trials. A similar correction is plausible for amycretin.
For more comparison context, the GLP-1 dosing comparison 2026 breaks down the approved and pipeline molecules side by side. The CagriSema REDEFINE Phase 3 guide covers the existing two molecule amylin plus GLP-1 combination that amycretin is conceptually replacing. The mazdutide Phase 3 evidence summarizes the GLP-1/glucagon dual agonist that is already approved in China.
Note: None of the head-to-head pairs above were tested in the same trial. Any rank order across drugs is provisional until a head-to-head readout exists. Phase 3 amycretin trials are placebo controlled, not active comparator controlled, in their first readouts.
Safety and tolerability so far
Adverse events with amycretin tracked the GLP-1 plus amylin class profile. The most common treatment emergent events in both the subcutaneous and oral programs were gastrointestinal: nausea, vomiting, decreased appetite, and constipation. Most events were mild to moderate and resolved during the dosing period. Less than 1 percent of subcutaneous participants discontinued treatment for adverse events at the top dose. Treatment discontinuation rates in the oral arm fell in the same range as the published oral semaglutide trials.
That profile matches the dual mechanism precedent. In REDEFINE 1, gastrointestinal events were reported by 72.5 percent of CagriSema participants versus 34.4 percent on placebo. Combining two appetite suppressing pathways in one molecule does not eliminate the gut side effects of either pathway. It packages them into a single titration schedule and a single injection site or pill schedule.
What the Phase 1 program cannot say: how amycretin behaves in adults with type 2 diabetes (the Phase 2 type 2 diabetes trial reported topline positive in November 2025 but is not yet peer reviewed), how it performs against an active GLP-1 comparator in the same trial, or whether the higher subcutaneous doses can be tolerated as steady state maintenance rather than escalation peaks. All three questions are being addressed in the Phase 3 program.
What the Phase 1 data do not establish
Numbers in the 20+ percent range drive premature treatment decisions. A few things to keep in mind before the Phase 3 readouts arrive.
The subcutaneous trial reached its top dose by escalation. Steady state maintenance at 60 mg has not been characterized in a published trial. The oral trial ran 12 weeks. Weight loss curves in this drug class do not flatten in 12 weeks. The peer reviewed numbers are short term proof of concept, not long term outcome data.
Cardiovascular outcome data do not exist. Semaglutide cleared SELECT for a 20 percent MACE reduction in adults with established cardiovascular disease and overweight or obesity, currently the gold standard outcome signal in the class. The semaglutide SELECT cardiovascular MACE evidence covers that data set. Amycretin will need its own outcome trial to make any analogous claim. None has been registered.
Kidney outcome data are also absent. Semaglutide cleared FLOW for kidney disease progression, covered in the semaglutide FLOW trial CKD evidence. Amycretin has no kidney data set.
MASH biopsy data are not available either. Tirzepatide cleared SYNERGY-NASH Phase 2 with 62 percent MASH resolution at 15 mg, covered in the tirzepatide MASH SYNERGY-NASH evidence. Amycretin has no liver biopsy program at this stage.
Head to head comparisons are missing. The Phase 1 trials used placebo controls, not active comparators. The Phase 3 program will be a placebo controlled obesity trial in its first readout, not a head to head with tirzepatide, retatrutide, or CagriSema.
Practical context for researchers
Amycretin is not commercially available in any market. It is not approved by the FDA, the EMA, the MHRA, or any other regulator. The molecule is in the investigational pipeline at Novo Nordisk. There are no compounded versions; the molecule structure has not been disclosed at a level that would support reverse synthesis, and compounding rules in the United States already exclude novel patent protected molecules.
If the interest is in the underlying GLP-1 plus amylin biology, the closest research available compounds are semaglutide (the GLP-1 half) and cagrilintide (the amylin half). The two molecule combination CagriSema is what Phase 3 amycretin will most directly compete with, and the REDEFINE 1 and REDEFINE 2 readouts are the closest current evidence of what dual pathway pharmacology produces in long term trials. Cagrilintide is available for research purposes from Ascension Peptides with 50% off using code ENHANCED, and semaglutide is available from the same source under research use disclosures.
Bottom line
Amycretin is the first test of GLP-1 plus amylin combined biology in a single molecule. Two Lancet papers in 2025 read out positive Phase 1 data in both injectable and oral formats. The headline weight loss numbers are competitive with the strongest existing drugs in the class, although the trials were small, short, and not head to head. Phase 3 enrollment opened in the first quarter of 2026 and is expected to take the same multi year readout timeline that other obesity Phase 3 programs follow.
For now, the appropriate reading is that amycretin is a credible candidate to compete with tirzepatide and CagriSema in late stage obesity trials. It is not a clinical option for anyone today and will not be for at least two to three years even on the fastest regulatory path. The CagriSema data set is the cleanest current proxy for what dual GLP-1/amylin pharmacology produces in a registrational trial.
References
- Safety, tolerability, pharmacokinetics, and pharmacodynamics of the first-in-class GLP-1 and amylin receptor agonist, amycretin: a first-in-human, phase 1, double-blind, randomised, placebo-controlled trial. Lancet. 2025. PMID 40550229
- Amycretin, a novel, unimolecular GLP-1 and amylin receptor agonist administered subcutaneously: results from a phase 1b/2a randomised controlled study. Lancet. 2025. PMID 40550231
- Lau DCW, Erichsen L, Francisco AM, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. Lancet. 2021;398(10317):2160-2172. PMID 34798060
- Walker CS, Aitken JF, Vazhoor Amarsingh G, et al. Amylin: emergent therapeutic opportunities in overweight, obesity and diabetes mellitus. Nat Rev Endocrinol. 2025;21(8):482-494. PMID 40360789
- Chapman I, Parker B, Doran S, et al. Effect of pramlintide on satiety and food intake in obese subjects and subjects with type 2 diabetes. Diabetologia. 2005. PMID 15843914
- Frias JP, Davies MJ, Albert L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2.4 mg with once-weekly semaglutide 2.4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet. 2023. PMID 37364590
This article is for educational and research purposes only. None of the content above constitutes medical advice. Amycretin is an investigational compound and is not approved by the FDA, EMA, or any other regulatory body for any indication. The numbers above describe what published Phase 1 trials measured under controlled conditions in fewer than 300 humans across short durations. They do not establish efficacy or safety for any specific individual and they are not protocols. Cagrilintide and semaglutide are sold under research use disclosures and are not for human consumption. Decisions about weight management belong with the patient and a qualified clinician.